

The Creation of the Prosthetic Finger is Challenging Enough
Creating prosthetic fingers on a daily basis is a challenge for anaplastologists on many levels. Its is a matter of the large commitment of time to design, fabricate, fit, check, and deliver. Each one of these areas account for hours of time. Then there are the patient and family expectations, all the emotional aspects of not only the appearance and functionality of the device but the person still recovering and accepting the loss of a body part. Also, other tangential things like impact on occupational opportunities and financial concerns, guilt of family members that maybe were involved in some way, fear of reentering social circles with friends, relatives, and plans to meet new people and have intimate relationships.
Anaplastologists deal with a lot taking on finger amputee clients of all ages. But when it comes time to get down to business and get a device made and delivered, we always find ourselves wondering, how could we make the prosthesis better. We say to ourselves and to the patient, yes, I will make it look convincingly real so “people will never notice it.” That is our patient’s primary goal and the goal we are most comfortable focusing on. But there are so often lingering thoughts, like, the prosthesis is so inanimate. Yes, we know the solid molded silicone rubber is the most durable design and material, essentially accepted as the “standard of care” in the prosthetics realm. However, we wish it mimicked actual anatomical complexity with a rigid skeletal-like core and a softer more flesh-like outer areas for natural feel. And it just flops around suspended to the segment of the finger that remains.
The Prosthetic Finger from the Biomedical Engineering Point of View
So, every now and then we at Medical Art Prosthetics try new designs. We commit even larger commitments of time, energy and costs to try something different. In our labs that is one thing. And when we have a willing patient to help us try new designs it can be very fun and fulfilling when we see promise, especially if the work and final device prove to be an improvement over a conventional “standard of care” designed device. These projects were prompted by the rather surprisingly successful flexing prosthesis delivered last fall in Tampa, Florida seen here:
What follows is another in a series of projects Medical Art Prosthetics. Our latest project with the University of Wisconsin biomedical engineering students produced yet another iteration of potential advances in prosthetic finger designs. Read how some of the brightest young engineering minds interpret our challenges and synthesize possible refinements to improve the prosthetic finger’s performance.
Biomedical Engineers of the Future Tackle the Challenges of Prosthetics
One semester’s progress is handed off to the Next’s like a baton in a race
Thanks to the last group seen below there was a healthy flow of ideas and progress for this Spring of 2026’s group to delve into and work from. They came up with some great designs for the prosthetic finger.

UW BME students Fall 2025
UW BME students Spring 2026
Spring 2026 Prosthetic Finger Project:
Introduction
A comprehensive systematic review shows that upper-limb amputations are a significant component of global amputations and that upper-limb trauma affects people of all ages, especially those in the working population [1]. Other estimates indicate millions of people worldwide require prosthetic/orthotic devices, yet only about 10% ever receive them, demonstrating a huge unmet need in assistive technology access [2]. 185,000 people have an amputation each year, which corresponds to about 300-500 amputations every day. According to the American Orthotic and Prosthetic Association, partial amputations and finger amputations represent the majority of upper-limb losses [2]. The client’s patient with a partial middle finger amputation notices their silicone prosthetic causes the most attention during a professional handshake or setting. Silicone prosthetic fingers often lack natural-looking joint movement and decrease the comfort and confidence for most patients [3]. Fabricating a finger prosthetic inserted into a silicone sleeve can improve the natural movement of the DIP and PIP joints, creating an overall more realistic-looking prosthetic finger.
Existing Devices
Several existing prosthetic finger designs illustrate the current approaches to restoring partial finger function. Commercially available body-powered devices, such as the MCP Driver® and PIP Driver® utilize passive mechanical linkages driven by residual joint motion to enable articulation at missing joints, providing improved grip stability and multiple grasp patterns without active actuation. The MCP Driver® is a commercially available body-powered prosthetic finger designed for amputations through the proximal phalanx. It uses residual motion at the metacarpophalangeal (MCP) joint to drive motion of the distal links in the finger. This body-driven design enables passive flexion and extension without electrical actuation, thereby improving grip stability and enabling multiple grasp patterns [4]. The PIP Driver® is another body-driven prosthetic finger device targeting replacement of the proximal interphalangeal (PIP) joint. Like the MCP Driver, it uses mechanical linkages and body motion to enable flexion at the missing joint. Although less widely marketed than the MCP Driver, its existence demonstrates the viability and interest in passive mechanical prostheses [4].

Figure 1: MCP Driver Prosthetic Finger [4,5]

Figure 2: PIP Driver Finger Prosthetic [6]

Figure 3: Knick Finger Prosthetic [7]
1.1 Problem StatementFinger amputations significantly reduce hand dexterity and the ability to perform everyday tasks, while current prosthetic fingers often provide primarily cosmetic restoration with limited functional benefit. Many silicone prosthetic fingers lack internal articulation and therefore do not replicate the natural flexion and extension of anatomical joints, resulting in stiff, unrealistic motion and minimal contribution to grip or object manipulation. Existing functional prosthetic finger devices may restore movement but can require sufficient residual anatomy, may not integrate seamlessly with cosmetic silicone sleeves, or may compromise aesthetic appearance. For patients with partial finger amputations and limited residual length, there is a need for a prosthetic solution that combines cosmetic realism with improved mechanical functionality. This project aims to design and fabricate a rigid internal prosthetic finger core with an integrated hinge mechanism that attaches to the patient’s residual finger and is mechanically coupled to the adjacent finger, enabling passive, synchronized flexion and extension that more closely mimics natural finger motion while maintaining a realistic external appearance.
I. BACKGROUND
2.1 Physiology and Biology
The human finger is composed of three phalanges the proximal, middle, and distal phalanges which articulate at the metacarpophalangeal (MCP), proximal interphalangeal (PIP), and distal interphalangeal (DIP) joints [8]. Flexion occurs when these tendons shorten, pulling the phalanges toward the palm. Extension occurs when extensor tendons on the dorsal side of the finger lengthen and pull the finger back into a straight position. The relationship between tendon excursion (movement distance), applied force, and joint angle is nonlinear, demonstrating the complex biomechanical interaction between muscles, tendons, and joints [9]. Proper articulation at the PIP and DIP joints is essential for maintaining grip strength, dexterity, and coordination. Disruption to these joints, such as joint fusion or amputation, alters motion patterns and reduces functional performance. Even small changes in tendon length or joint mechanics can significantly affect finger motion, highlighting the importance of precise mechanical design when restoring function [10].
2.2 Prototype Design and Fabrication
Polylactic acid (PLA) was selected as the primary structural material for the prosthetic finger core due to its favorable mechanical properties, biocompatibility, and compatibility with additive manufacturing. PLA exhibits tensile strength values ranging from approximately 40–70 MPa and a Young’s modulus of about 2–4 GPa, indicating sufficient stiffness and strength to withstand moderate mechanical loading while maintaining structural integrity [11]. Additionally, PLA is widely used in biomedical applications because it is biocompatible and degrades into non-toxic byproducts, making it suitable for devices that interact with the human body [12]. Its compatibility with fused deposition modeling (FDM) allows precise fabrication of complex geometries and customized components, which is essential for
patient-specific prosthetic designs [12]. Stainless steel components were incorporated for hinge joints and force transmission because stainless steel provides high strength, stiffness, and excellent corrosion resistance, enabling reliable mechanical performance under repeated loading conditions [13]. The combination of PLA for lightweight structural support and stainless steel for load-bearing articulation enables the prosthetic finger to achieve durability, functionality, and patient-specific customization.
2.3 Client Information
The client for this project is Greg Gion, an anaplastologist at Medical Art Prosthetics, LLC who specializes in the design and fabrication of custom silicone prostheses. He is collaborating with the team to develop a functional internal prosthetic finger core that integrates with a cosmetic silicone sleeve to improve both the motion and realism of a patient’s middle finger prosthesis.
2.4 Design Specifications
The Product Design Specification defines the functional, mechanical, anatomical, and usability requirements for the flexing prosthetic finger core (see Appendix [A] for full PDS). The device must provide passive flexion and extension at the proximal and/or distal interphalangeal joints through a low-resistance hinge mechanism, allowing motion driven by the adjacent finger. It must securely attach to approximately 1.5 cm of the patient’s residual finger and interface with the
adjacent finger without causing discomfort, irritation, or restricting natural movement. The prosthetic core must be rigid enough to provide structural support while fitting within a cosmetic silicone sleeve and remaining lightweight and unobtrusive. Biocompatibility, durability under repeated daily use, and compatibility with 3D scanning and additive manufacturing processes are required. Additionally, the design must maintain anatomical realism, minimize visibility of mechanical components, and allow integration with existing prosthetic fabrication workflows at Medical Art Prosthetics.
II. PRELIMINARY DESIGNS
3.1 Design 1: Hinge Joint
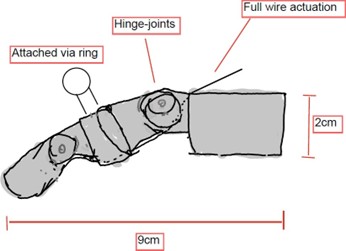
Figure 4: Hinge-Joint Design
The hinge-jointed design consists of a finger body based on the Knick-Finger open-source prosthetic. It features two hinge joints, an attachment sleeve for the residual finger, wire-actuated bending, and a silicone ring attachment for the adjacent finger. This design aims to improve the prosthetic’s compatibility with the silicone cover by minimizing sharp edges using round hinges and a sleek body. The body is fully 3D printed from PLA using the Knick-Finger template and allows a tendon-like wire to be passed through all joints for anatomically accurate finger bending. The hinge-jointed design is meant to look more similar to a real finger skeleton than the current gear-based design of last semester. The silicone ring attachment is inconspicuous and lets the user manipulate the prosthetic with their adjacent finger up to the fingertip, which can be moved using the wire. Overall, this design prioritizes anatomical accuracy, sleeve compatibility, and ease of fabrication.
3.2 Design 2: Bar-Linked
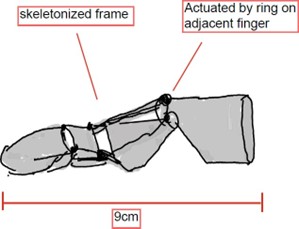
Figure 5: Bar-Linked Design
The bar-linked design’s most notable features are its linked bar connectors that are used to manipulate the joints in a movement that is anatomically similar to a real finger, although it is not as accurate as a “tendon”. The bar linkage offers this design unique advantages, such as structural stability due to the rigid bars, while maintaining a low profile due to the flatness of the bars. The bar-linked design also makes use of adjacent finger actuation using the silicone ring attachment. Manipulating the middle segment of the prosthetic using the adjacent finger leads to full finger bending due to the linkage of the bars. This design may also be completely 3D printed, but will have more small individual parts than the
hinge-jointed design. The bar links allow for more space between the sides of the joint, minimizing body material usage.
3.3 Design 3: Skeleton Frame
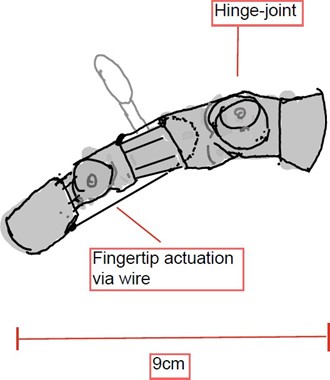
Figure 6: Skeleton-Frame Design
The skeleton frame design is meant to reduce the amount and volume of solid material inside the silicone finger sleeve. This design uses hinges that are composed of slender frames connected by pins to move two finger joints. The minimalistic structure provides a solid but unobstructive frame for the finger, and empty space could be filled with foam or other soft material to provide a more realistic texture to the prosthetic finger. This prosthetic is also designed to actuate with the adjacent finger via a silicone ring. The skeleton frame design is efficient in the use of space and material, but it sacrifices anatomical accuracy. The design does not have the cylindrical structure of real finger bones and is not tendon-actuated, potentially making movement less natural compared to a hinge-jointed design.
III. PRELIMINARY DESIGN EVALUATION
4.1 Design Matrix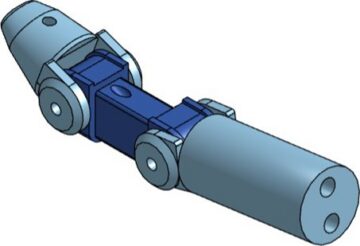
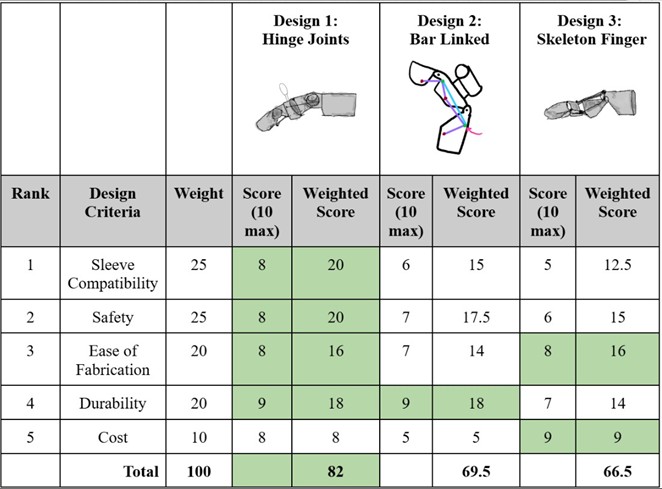
Table 1: Prosthetic Finger Mechanical Core Design Matrix
The design matrix evaluates three possible designs based on five criteria, which are presented in order of importance. Sleeve compatibility and safety are ranked as the most important categories. The hinge joint design won the sleeve compatibility category due to its rounded shape and a lesser increase in joint surface area upon bending. The hinge joint design is the most anatomically similar to real finger bones and is therefore more compatible with the sleeve. The hinge joint design also won the safety category due to its lower mechanical complexity and more predictable motion compared to the other designs. The other designs used smaller-sized parts and raised more structural stability concerns. In the ease of fabrication category, the hinge and skeleton designs are tied due to them both being fully 3D printable with minimal, small disconnected parts. In the durability category, the hinge design came into a tie with the bar-linked design due to the latter’s rigidity, which increases its durability, while the hinge design’s simple mechanics keep it safer from failure. The skeleton design’s lack of material is reflected in its lower durability score. Finally, the skeleton frame design wins the cost category due to being fully 3D printed and having the least amount of material.
4.2 Design Matrix Criteria Analysis
Sleeve compatibility (25): This category evaluates how well this device would interact with the silicone sleeve provided by our client. This is a high priority as the main purpose of this project is to create an aesthetic prosthetic for a patient which requires the sleeve for the device to appear like a natural human finger. The issue with the last solution was that the core did not fit well into the silicone sleeve which is how this criteria was developed. In our analysis of the designs, sleeve compatibility favored the hinge-based design due to its compact, axially aligned geometry and predictable motion envelope. Ranked lower than this was the bar-linked system which introduced additional lateral components requiring increased internal clearance. The joints of the bar-linked design would have to have a range compatible with the amount the finger needs to bend and would have more possible points to stretch the sleeve. Finally, the skeleton design presented irregular geometry and potential stress concentrations within the silicone sleeve, reducing its compatibility.
Safety (25): This category evaluates how safe this device would be for manufacturing, and use by the patient. The
hinge-based design presented the lowest mechanical complexity and most predictable motion, reducing pinch points and structural failure risk which is why it is ranked highest in this category. Next, the bar-linked design introduced additional moving components, increasing pinch and failure risk. Finally, the skeleton design ranked last for safety. While the skeleton design is simple, it presents potential brittleness and internal stress concentration concerns, lowering its overall safety rating. As none of these designs are internal or directly interact with the patient’s skin overall safety risk is low.
Ease of Fabrication (20): This category evaluates how well the design can be fabricated and made with the materials we have available to us. This is an important criteria as without the ability of manufacturing the design, we have no way to test it and see if it works and no models to give to the client. As 3D printing is a fast, feasible way of making prototypes and models the hinge joints design and the skeleton finger design are both rated highly. The primary concern with these two designs is ensuring that the prints come out how we intended and ensure our designs can be accurately depicted in CAD. The bar-linked design scored lower because this design is most likely not going to be 3D printed, or at least not entirely 3D printed. This design could include the use of metal bars and a flexible casing to separate the bars from the silicone sleeve. For the additional materials and assembly requirements the bar-linked design was ranked last.
Durability (20): This category evaluates how well the prosthetic holds up through daily wear and tear. The prosthetic needs to be able to withstand thousands of bending cycles a day without compromising the functionality and natural appearance of the finger. The skeleton finger design presented the lowest durability with a score of 7 due to its complex structure that could cause weakening of the silicone sleeve. Additionally, the components are very thin which could lead to early weakening of the prosthetic. The hinge-based and the bar linked designs both scored a 9 in terms of durability. This is because both designs offered minimal exterior protrusions that could lead to weakening of the silicone sleeve, and also offered solid cores and reliable joints that can withstand the forces that come with daily usage.
Cost (10): This category evaluates the expenses that would be incurred by each design. Many current prosthetics are very expensive so the design should work toward an inexpensive solution, this makes cost an important criteria to consider.
Based on the designs, the two 3D printed designs rank much higher than the bar-linked design. The skeleton finger design ranked first as this design can be entirely 3D printed in separate parts allowing for low cost primarily depending on the material the design is printed in. The skeleton finger design ranked higher than the hinge joints design as it covers less surface area and thus will cost less to print. The hinge joints design can also be primarily 3D printed with the addition of a string or wire connecting the two joints which incurs little extra cost. The bar-linked design ranked last as this would have the most non-3D printed components. The bar-linked design could be constructed using metal bars and joints with the addition of a shell to fill extra space, and protect the joints and silicone sleeve. Overall, a fully 3D printed design will most likely be less expensive than a multi-component meta, base, and casing design.
4.3 Proposed Final Design
Figure 7: Proposed Final Design of Mechanical Core
The hinge-joint design was ultimately selected as the winning design from the design matrix and as the proposed final design. This design’s anatomical accuracy, combined with its relative mechanical simplicity and high durability, makes it the best design for our application out of the three. The hinge design won or timed in every category other than cost, which is the most negligible category due to cost being a few cents for 3D printing and then a small amount for any pins that might be purchased. This design had no major weaknesses or tradeoffs and is well-rounded in all important aspects for our prosthetic design requirements. The final proposed hinge design is slightly different from the original hinge design, with an even slimmer body due to the removal of the mid-joint bumper, which was a remnant from the Knick-Finger. The base of the prosthetic is also adjusted to be shorter since the user’s residual finger is not meant to be inserted into the mechanical prosthetic, which would be fitted on a finger cap. Lastly, the location of the actuation wire is changed to only move the fingertip, as the silicone ring will move the other joint. Overall, the other two designs were too specialized in specific areas and lacking in others, which gave the all-rounder design the winning score.
IV. FABRICATION
5.1 Materials
The prosthetic finger mechanical device will be 3D printed out of PLA plastic, due to its high strength properties [14]. It will also contain stainless steel dowels to hold the hinge joints in place, as well as have a stainless steel cable for potentiating the finger tip. Stainless steel is very corrosive resistant and durable which makes it the perfect metal choice [15]. The team also needs to research what mechanism we need to use in order to secure both ends of the wire and dowels. The outer sleeve will be made of silicone which will be constructed by our client.
5.2 Methods
Given the complex nature of the design, the fabrication process must be precise. The stainless steel components will be ordered online and should be manufactured to the sellers specifications. The 3D printed parts will need to be printed with as much detail as possible. We will use the BambooLabs 3D Printers at the Makerspace with the “Fine” printing speed setting and a 25% honeycomb infill pattern, in order to maximize both strength and design integrity. Some post printing cleanup might be necessary, which would be completed using hand tools if needed. In terms of assembly, the parts need to be carefully assembled so that all moving parts are free from blockages and effectively stay in place.
5.3 Final Prototype
The final prototype consists of two hinge joints connected to a simulated middle phalanx, which in turn connects to a base and fingertip attachment. The stainless steel dowels will hold the hinge joints in place, while the wire attaches to the top of the base, runs down through the middle phalanx, and then is secured to the bottom of the fingertip.
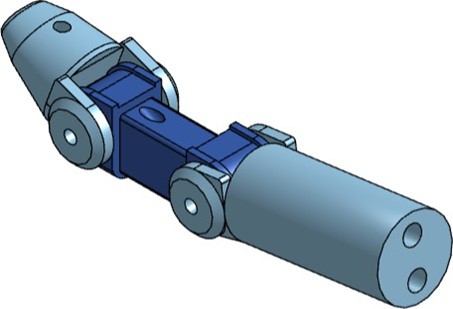
Figure 8: Final fully assembled prototype of the prosthetic finger
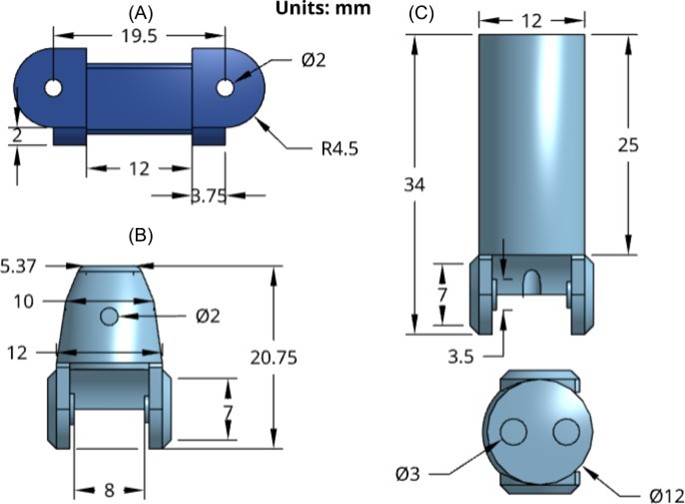
Figure 9: (A) highlights the middle phalanx dimensions (B) shows the fingertip dimensions (C) displays the finger base dimensions
5.4 Testing
No testing has been completed as of now, however, future plans include:
Range of Motion Testing
The PIP and DIP joint flexion angles will be measured using a goniometer when the prosthetic is inside the silicone sleeve. These values will be compared to those of a nonamputated human finger to test how anatomically accurate the prosthetic is. The data will be compared using a paired t-test to see if the prosthetic range of motion differs significantly from the nonamputated human finger.
Accelerated Life Testing
The prosthetic will be run through 3000 cycles, one cycle meaning going from strait to bent back to strait, with progress being tracked every 500 cycles. This will show if there are any weak spots in the design that need to be addressed, as well as if the prosthetic can withstand daily usage. This would also be coupled with MTS compression testing to see how much force the prosthetic can withstand. Although it doesn’t need to replicate the strength of an anatomical finger, it still should have decent durability. The PIP joint will be tested using a protocol outlined by Medical Art Prosthetics. Securing the prosthetic in place with a stage adapter, the finger will be tested in a fatigue test with the proximal segment of the prototype secured at a 45° angle to the MTS movement direction. Signs of wear after the fatigue test may be noted by observers, addressing failure modes [16].
Qualitative Task Based Pass/Fail Testing
Qualitative tests are necessary to evaluate the comfort and general ergonomic design of the prosthetic. The Anthropomorphic Hand Assessment Protocol (AHAP) evaluates the grasping abilities of upper-limb prostheses, including finger prosthetics. Common loading patterns will be evaluated, including tip pinch, pulp pinch, key pinch, and power grip [17]. Up to 26 tasks involving 25 household items may be used in a performance evaluation. Each task is then scored based on its grasping and holding ability by the user on a 0, 0.5, or 1 rating scale [18].
Such tests will be performed to evaluate the performance of the prosthetic finger in common loading patterns. The combination of quantitative and qualitative testing will provide an encompassing overview of the finger’s success, including the objective forces it can withstand and subjective comfort and usability. Conforming to desired force output thresholds and ergonomics will produce a prototype to meet client requirements. The team hopes to have the client’s patient run through this test once a fully functional prototype is developed.
5.5 Results
No results have been obtained, yet here are some potential outcomes:
Range of Motion Testing
Results should display a p value that shows no significant difference between the prosthetics and the nonamputated human fingers range of motion.
Accelerated Life Testing
The prosthetic should make it through all 3000 cycles with no noticeable damage and force values should reflect literature ranges as noted in Appendix A. A 10% range is expected between the dominant and nondominant hand [19].
Qualitative Task Based Pass/Fail Testing
Results should follow the rating scale described by Siegel et al [18]. Determination of passing or failing from the patients results of the test will result in further prototype modifications. Further, statistical analysis should be performed to evaluate the statistical significance of testing. This will include P-test and standard deviation analysis, as well as qualitative observations and comments.
V. DISCUSSION
The results of the testing can be related to relevant research in the finger prosthetics field. Research was done on the impacts of tripod and finger tip pinch using the Southampton Hand Assessment Procedure (SHAP) scale to see if mechanical prosthetic devices have a significant impact compared to silicone prosthetic devices [20]. The passive silicone prosthetics can decrease finger tip grip by about 10% so a net improvement of finger tip grip would show a positive effect of the mechanical prosthetic. Using this assessment procedure the team will use data collected from completing the SHAP test using the prosthetic to the results of a passive silicone prosthetic. In a different study, the grip of a healthy hand is measured to be about 148 N while an injured hand is about 120 N [21]. These force values can be compared to the forces of the prosthetic finger during mechanical testing to see the effects on overall grip strength and if the force has improved from the injured hand. The Anthropomorphic Hand Assessment Protocol (AHAP) provides a standardized protocol for testing human-like hand robotics and prosthetics[22]. In the protocol there are 26 tasks to test the most relevant human grasp types. Through these tests, healthy human hands have a 100% Grasping Ability Score (GAS), while the prosthetics ranged from scores of 45% to 79% [22]. The team will use these tasks and the average GAS score which is 62.5% to test the prosthetic against. The force values and real world assessment tasks are important aspects of current prosthetics that will help show the functionality of the prosthetic finger design.
Ethical considerations are important when considering research, testing, and use of prosthetic devices. It is important that the prosthetic design does not cause the patient discomfort or limit the remaining motion they have in their residual middle finger and actuating ring finger. The current prosthetic does not have the ability to bend but lacks a rigid core that may constrict the movement of the adjacent fingers. As the rigid core of the prosthetic will have no contact with the patient it is important to ensure the silicone and portions of the prosthetic that are in contact with the client’s skin are biocompatible and do not cause irritation to the skin. The prosthetic must be easily removable by the patient to ensure the patient’s comfort and ability to clean the prosthetic. Outside of the physical prosthetic, insurance is a key factor in the prosthetics field as they can be expensive and not otherwise accessible without insurance. A key factor for insurance is that the device is deemed “medically necessary” meaning the prosthetic must restore or improve function of daily activities, address a diagnosed condition, improve independence, or prevent further injury. For finger prosthetics these criteria can be met by providing support for gripping and fine motor tasks however some prosthetic devices such as silicone prosthetics and cosmetic elements are deemed non-essential unless they are combined with functional components [23]. These many concerns will be taken into consideration when designing and manufacturing the prosthetic device to ensure the compatibility with patients as well as accessibility through insurance.
Evaluation will allow the team to identify changes to the design that need to be made. Changes can be identified by the physical evaluation, visual inspection, and patient feedback. Visual inspection is a key initial evaluation when combining multiple parts. In the case of the rigid mechanical core and the silicone sleeve, seeing that the joints of the core limit the bending of the silicone can cause evaluation of the joint design. The mechanical testing may show force values lower than the value that is set as the minimum acceptable value for the prosthetic which can result in reevaluation of the materials chosen and possible changes to the design as well. Many of these testing and areas for evaluation can also be sources of error. Patient feedback is a key evaluation point but the patient will not be present for primary testing thus mechanisms must be developed to simulate the force and positions of the patient’s finger motion. This increases the chance for inconsistencies in how the force, flexion, and extension are measured as the mechanism may not accurately replicate how the patient will use the prosthetic in daily use. Further limitations may occur in the SHAP and AHAP grip assessments without the patient performing the tests. Alternate testing methods must be used which may result in discrepancies between what is observed while testing and the prosthetic’s performance in the patient’s real-world application. These sources of error must be taken into consideration when looking at the results gathered from the tests performed on the prosthetic.
VI. CONCLUSIONS
This project aims to design and develop a rigid core to be integrated into a silicone prosthetic finger sleeve. The core is designed to provide natural flexion and extension to a silicone prosthetic, that is otherwise passive, while maintaining the life-like appearance of the prosthetic. The prosthetic design will provide increased function and support to activities the patient does daily including gripping, holding, and pinching. The final design utilizes hinge joints which will allow the silicone sleeve to bend as the hinges are actuated by the adjacent ring finger. The hinged joints will limit the increased surface area of the rigid core in the bent position allowing it to bend within the restrictions of the silicone sleeve. The design will allow the natural bending of the patient’s adjacent ring finger to cause flexion in the PIP joint and a tendon-like wire to actuate bending at the DIP joint of the prosthetic. This chain of motion results in a natural coordination of joint bending aligning with the bending of the adjacent ring finger.
Through the completion of mechanical force testing and effectiveness assessments using the Southampton Hand Assessment Procedure (SHAP) and Anthropomorphic Hand Assessment Protocol (AHAP) the team hopes to provide significant evidence of the prosthetic finger meeting design requirements and performance expectations. The mechanical force testing will provide numerical evidence of the forces the prosthetic can withstand which will be compared to literature values of healthy human fingers. This will support the ability of the prosthetic to perform functional activities and durability claims. The SHAP and AHAP assessments will help the team determine a Grasping Ability Score (GAS) and evaluate the ability of the prosthetic finger to function in common grasp types. The data collected through these tests will help determine the effectiveness of the prosthetic finger which the team will draw performance conclusions from.
The next steps for this project include determining the materials needed, finalizing the design, and developing the design in 3D CAD software. As 3D printing is a primary mode of fabrication, determining the proper print settings is also an important step as they affect the print durability and function of the prosthetic. Looking forward, the team will continue working with our client Mr. Gion to ensure the design is consistent with the design requirements and meet Mr. Gion’s expectations. Further work in this project includes looking into the customizability of the prosthetic. Finger amputations occur at various locations on the finger and include the loss of different amounts of joints and phalanges, creating a more inclusive or customizable design creates a larger number of patients that can benefit from the prosthetic design.
Approaches to creating a more customizable design include adding an electronic component to aid in actuation of the prosthetic and produce independent motion, this would negate the need for an adjacent finger to actuate the prosthetic and allow for single joint prosthetics focusing on the DIP joint. These additional considerations introduce difficulties to be addressed after there is a working prototype for the specific patient the team was tasked to develop a prosthetic for. Once the product is finalized it will begin going through testing with the prospect of the device being used by the patient and further developed into a customizable finger prosthetic design.
VII. ACKNOWLEDGEMENTS
The team would like to extend our appreciation to Mr. Greg Gion at Medical Art Prosthetics for inspiring and supporting this project. Additionally the team would like to thank Dr. Justin Williams and Caelen Nickel for their guidance and support throughout this project.
VIII. REFERENCES
- Z. Rahman et al., “Global Lower and Upper Limb Amputation: A Literature Review,” Cureus, vol. 8, no. 12, p. e719, Dec. 2016. [Online]. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4864250/
- S. Waldman, “Prosthetic challenges: why access to prosthetic and orthotic devices remains low worldwide,” ALT Blog, Apr. 16, 2024. [Online]. Available: https://www.3dalt.com/altblog/2024/4/16/prosthetic-challenges [Accessed: 25-Feb-2026].
- Rathod et al., “Silicone finger prosthesis for a partially amputated index finger – A case report,” Journal of Cardiovascular Disease Research, 2021.
- “MCPDriver,” Naked Prosthetics Devices, Prosthetic [Online]. Available: https://www.npdevices.com/devices/ (accessed Feb. 25, 2026).
- “MCPDriver,” Naked Accessed: Feb. 17, 2026. [Online]. Available: https://www.npdevices.com/devices/mcpdriver/
- “PIPDriver™ – Body-Driven Prosthetic Finger,” London Prosthetics [Online]. Available: https://www.london-prosthetics.com/prosthetic-solutions/upper-limb/naked-prosthetics/pipdriver%E2%84%A2/ (accessed Feb. 25, 2026).
- “Knick Finger,” Enabling The Future, May 2, [Online]. Available: https://enablingthefuture.org/2016/05/02/knickfinger/ (accessed Feb. 25, 2026).
- Bouredoucen, S. Boudabbous, P.-A. Poletti, and L. Taihi, “Metacarpophalangeal joints of the long fingers: Anatomy, biomechanics, and imaging techniques,” European Journal of Radiology, vol. 194, p. 112459, Jan. 2026, doi: 10.1016/j.ejrad.2025.112459.
- Zhang and Y. Xiong, “Biomechanical study of flexor tendon and finger motor function,” Sheng Wu Yi Xue Gong Cheng Xue Za Zhi (Journal of Biomedical Engineering), vol. 26, no. 6, pp. 1267–1270, Dec. 2009. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/20095484/
- P. Schweitzer and G. M. Rayan, “The terminal tendon of the digital extensor mechanism: Part II, kinematic study,” Journal of Hand Surgery, vol. 29, no. 5, pp. 903–908, Sep. 2004, doi: 10.1016/j.jhsa.2004.04.025. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/15465242/
- Farah, D. Anderson, and R. Langer, “Physical and mechanical properties of PLA, and their functions in widespread applications — A comprehensive review,” Advanced Drug Delivery Reviews, vol. 107, pp. 367–392, Dec. 2016. Available: https://pmc.ncbi.nlm.nih.gov/articles/PMC7474829/
- Tao, H. Cheng, L. Liu, and Y. Zhao, “Additive manufacturing of biodegradable polymers for biomedical applications,”
- Polymers, vol. 16, no. 1, 2024. Available: https://pmc.ncbi.nlm.nih.gov/articles/PMC11694096/
- Davis, M. Chen, and J. Smith, “Mechanical properties and corrosion resistance of stainless steel for biomedical applications,” Materials Science and Engineering C, vol. 70, pp. 123–131, Jan. 2017. Available: https://pmc.ncbi.nlm.nih.gov/articles/PMC5583085/
- Ruitai Mould, “Polylactic Acid(PLA)| What Is It, Properties, Types, & Use,” Ruitai https://www.rtprototype.com/what-is-pla/
- Eagle Stainless Tube & Fabrication, , “Eagle Stainless Stainless Steel Characteristics,” eagletube.com, 2022. https://eagletube.com/about-us/news/stainless-steel-characteristics/
- Chaudhry, K. Fetsch, B. Loi, and J. Riley, “Development of a fully actuated realistic finger prosthesis for proximal phalanx amputations,”
- Y. S. Chao, K-N. An, P. Cooney, and R. L. Linscheid, Biomechanics of the Hand. World Scientific, 1989.
- R. Siegel, M. A. Battraw, E. J. Winslow, M. A. James, W. M. Joiner, and J. S. Schofield, “Review and critique of current testing protocols for upper-limb prostheses: a call for standardization amidst rapid technological advancements,” Frontiers in robotics and AI, vol. 10, Nov. 2023, doi: https://doi.org/10.3389/frobt.2023.1292632.
- C. Roberts et al., “A review of the measurement of grip strength in clinical and epidemiological studies: towards a standardised approach,” Age and Ageing, vol. 40, no. 4, pp. 423–429, Jul. 2011.
- “Impact of silicone prosthesis on hand function, grip power and grip-force tracking ability after finger ” Accessed: Feb. 23, 2026. [Online]. Available: https://oce-ovid-com.ezproxy.library.wisc.edu/article/00006479-201640060-00012/PDF
- “Influence of finger amputation on grip strength and objectively measured hand function: a descriptive cross-sectional study.” Accessed: 23, 2026. [Online]. Available: https://oce-ovid-com.ezproxy.library.wisc.edu/article/00004356-201506000-00012/PDF
- Llop-Harillo, Pérez-González, J. Starke, and T. Asfour, “The Anthropomorphic Hand Assessment Protocol (AHAP),” Robotics and Autonomous Systems, vol. 121, p. 103259, Nov. 2019, doi: 10.1016/j.robot.2019.103259.
- “Are finger, hand, and thumb prosthetics covered by insurance? – Finger ” Accessed: Feb. 23, 2026.
IX. APPENDICES
10.1 Appendix A – Product Design Specification
Product Design Specifications
Date: 02/05/2026
Project Title: Flexing Prosthetic Finger Potentiated by Adjacent Finger
Team: Jack Zemlock, zemlock@wisc.edu – Team Leader/BPAG Sydney Smith, slsmith42@wisc.edu – Communicator Yair Ben Shaul, benshaul@wisc.edu – BSAC
Emma Hellberg, ehellberg@wisc.edu – BWIG
Client: Mr. Greg Gion
Advisor: Prof. Justin Williams
Function
Prosthetic fingers are often designed primarily for cosmetic purposes, offering limited functionality. They typically lack natural bending motion and cannot support weight during movement. The goal of this project is to design and fabricate a rigid internal core for a patient’s middle finger prosthesis, to be used in conjunction with an existing flexible silicone sleeve. The prosthetic will incorporate a hinge mechanism at the natural joint to enable flexion and extension, allowing for more lifelike motion. It will attach to both the remaining 1.5 cm of the patient’s residual finger and the adjacent ring finger. The primary objective is to restore functional movement that closely mimics natural finger motion while maintaining an aesthetically realistic appearance.
Client requirements
- The client is requesting an innovative way to give a silicone model of a flexible prosthetic middle finger a lifelike animation by creating a mechanical inner core.
- The client requires that the design fit with the size of the existing prosthetic and be narrower than the silicone sleeve interior and narrower than the previous design, see Size specifications.
- The client requires that the design not affect the aesthetics of the
- The client requests a way to give the finger enough functionality to qualify for insurance to cover the costs for the patient.
Design requirements
1. Physical and Operational Characteristics
- Performance requirements:
- The flexing prosthetic finger will be used every day, for the duration of 12 to 16 It will be taken off for cleaning and sleeping as the patient requires.
- The prosthetic will be potentiated by an adjacent finger; thus, it must be durable to stand up to common loading The finger must maintain one degree of freedom for both the distal interphalangeal joint (DIP) and proximal interphalangeal joint (PIP), to match the adjacent finger [1]. The finger must be flexible enough to maintain the patient’s full range of motion, such as flexing the hand into a fist and pointing a finger. The PIP joint must flex to a maximum of 120 degrees, and the DIP joint must flex to a maximum of 90 degrees [2].
- Daily use actions the finger may undergo include gripping, holding, pushing, and The prosthetic finger must not fail when faced with these tasks.
- The prosthetic must remain securely on the patient’s remaining limb without cutting off circulation. It must not fall off during the duration of use but is able to be removed by the patient after any duration.
- The prosthetic must function naturally with the silicone exterior provided by the client, Mr. Greg Gion, appearing realistic when applied to the hand of the patient.
b. Safety:
- The middle finger blood flow typically ranges from 1.07-1.46 ml/100 ml/s while resting [3]. The prosthetic finger must remain secure while maintaining proper blood flow to the finger. The prosthetic finger will be directly adhered to the hard silicone cap that attaches to the remaining finger. To ensure the health of the remaining portion of the finger, healthy blood flow should be maintained.
- The material interacting with the patient must be biocompatible and not irritate the patient’s The material must uphold the standard outlined in ISO 10993-10 for devices worn constantly as the prosthetic will be used daily [4].
- The prosthetic finger must be easily removable by the patient for cleaning, sleeping, and as the patient requires.
c. Accuracy and Reliability:
- The prosthetic finger should achieve similar common loading force values to a human finger in patterned movements such as pinch and grip actions so as not to fail while in use. The force values for natural pinch force range from 49 to 74 N (11.02 to 64 lbs). Natural grip force ranges from 80 to 540 N (17.98 to 121.40 lbs) [5].
- The finger should achieve similar flexion angles to a human finger. The PIP joint goes from 100° to 120° at full flexion and the DIP joint ranges from 80° to 90° at flexion [2]. The DIP joint should rotate about 0.76° for every 1° the PIP joint rotates [2]. The joint must not limit the flexion or extension of the adjacent finger.
- These flexion angles and force values should be maintained throughout the lifespan of the
d. Life in Service:
- The prosthetic finger will be worn for approximately 12-16 hours a day for the device’s life in service.
- The completed prosthetic device will have an average life in service of about 3 The different components have different lifespans with the silicone sleeve likely failing before the mechanical core.
- A silicone prosthetic finger can last 3 to 7 years although the thinner sleeve that will be used to encase the interior mechanical core will likely only last 2-3 years depending on the thickness and interaction between the mechanical core and sleeve material [6].
- The interior mechanical core will have a life span of about 3-5 years depending on the material and usage conditions [7].
e. Shelf Life:
- The prosthetic will spend most of the time being worn by the user, as it is custom-made for the user’s finger and therefore will spend little time in It could be set aside for sleep, where it will be exposed to normal room temperatures.
f. Operating Environment:
- The prosthetic finger would be exposed to skin temperatures on a regular This includes a range of 32–34 °C [8].
- The prosthetic would be exposed to the range of temperatures that a human hand would withstand safely, as it will be attached to the patient’s hand. Heat would be the main danger for components that may be made with plastic, which could experience temperatures of up to 38 degrees Celsius, which is around the upper acceptable range for human contact [9].
- The device will be covered with a silicone sleeve and should be able to withstand the compressive force applied to it.
- An appropriate temperature range could be determined once a material has been selected for the prosthetic.
g. Ergonomics:
- The prosthetic will be attached to the user’s residual finger with enough pressure to stay on securely and safely without cutting off the blood supply to the finger. The safe pressure range on the residual finger would be lower than about 5 N. [3]
- The device will be attached to the adjacent finger. Therefore, it will act with forces comparable to those produced by that This depends on the user’s grip strength.
Based on average grip strength for the patient’s age group, the prosthetic should support force values discussed above over the whole hand for full functionality. However, the loss of a finger will likely mean that the patient is not able to produce the same amount of force as a fully functioning natural human hand.
h. Size:
- The prosthetic is made to fit inside a silicone mold of the patient’s finger, and should therefore be slightly smaller than the full-size The average male middle finger is
75.5 ± 3.3 mm [20]
- The prosthetic should also have an attachment site that is the size of the residual finger for proper attachment.
i. Weight:
- The prosthetic should not feel noticeably heavy and should remain around the weight of a regular human finger which is around 18-22g.
j. Materials:.
- The prosthetic needs to be constructed out of a durable, sturdy material that is able to withstand daily wear and Metals provide a durable, strong material. However, they can lead to discomfort and corrosive metals like iron and zinc must be avoided.
- The material should mimic a typical finger range of Plastics such as polyethylene and polypropylene combined with a silicone rubber offer a sound balance between structural support and flexibility [10].
- A typical prosthetic needs to be easily customizable and adaptable; 3D printing provides customizable designs using materials such as SUV elastomers, acrylics, and various
k. Aesthetics, Appearance, and Finish:
- The prosthetic appearance needs to match that of a realistic finger, as well as blend in with the patient’s surrounding fingers to create a seamless, overall appearance [11].
- The color of the prosthetic should match the patient’s skin tone in order to look natural amidst the neighboring fingers.
- The prosthetic will include wrinkles, lines, and various patterns by using plaster cast models of the patient to add a more natural look [11].
- The finger will have a suitable core that allows for a natural feel when completing tasks such as shaking hands.
2. Production Characteristics
- Quantity:
- One prosthetic finger is required for the given patient, however, the design will take into consideration reproducibility to potentially expand the product to other patients.
b. Target Product Cost:
- The target product cost is under $1000 as given by the
- Existing passive silicone finger prosthetics start as low as a couple of hundred dollars from online retailers; however, more commonly the price range is $1000 to $5000 for a custom-fitted, color-matched product at a clinic or hospital [12].
- Manufacturing costs will be from the use of 3D printing, silicone and metal, likely stainless steel, for hinge and attachment The silicone will be obtained from the client’s pre-established supplier. Typically, a 2-lb silicone rubber or gel kit is upwards of
$50 [13]. With the potential to produce multiple prototypes, manufacturing costs should be between $100 and $200. Improvements to the design with the use of different materials will likely increase costs.
3. Miscellaneous
- Standards and Specifications:
- ISO 10993 is a widely used family of standards governing biocompatibility testing, which is crucial for any prosthetic material that contacts human tissue or Parts of ISO 10993 guide biological evaluation methods supported in FDA submissions [14 ].
- The U.S. Food and Drug Administration (FDA) regulates prosthetic devices as medical devices. Prosthetic fingers fall under general device classifications where regulatory controls depend on risk class (I/II/III). Devices in Class II typically require a 510(k) Premarket Notification, while higher-risk ones may require Premarket Approval (PMA) before The FDA also maintains a database of recognized consensus standards (ISO, ASTM) used to support compliance.
- The FDA product classification system includes specific product codes for prosthetic components, g., PROSTHESIS, FINGER, POLYMER (classed within device codes that may require a 510(k) depending on risk/exemptions) [15].
- ISO 8549 series defines terminology for external limb prostheses and orthoses, ensuring consistent naming conventions across documentation and regulatory submissions [16].
- ASTM International develops consensus test methods often recognized by the FDA. For example, ASTM documents may cover material properties, wear assessment, and mechanical testing relevant to prosthetic components. While some ASTM standards are specific to joint implants (e.g., hips), equivalent tests may be adapted for prosthetic finger materials and durability studies [16].
b. Customer:
- Desires a prosthetic solution that integrates seamlessly with the residual finger, allowing for natural, coordinated movement with the adjacent In particular, the prosthetic
should bend in unison with neighboring digits to support everyday hand gestures such as handshaking and pointing.
- Is dissatisfied with the rigidity of the current prosthetic, especially in situations where the surrounding fingers are flexed. Additionally, the customer would like a prosthetic appearance that provides a more natural and discreet look in professional settings.
c. Patient-related concerns:
- The client indicated that sterilization between uses is not required. However, the prosthetic should be durable enough to tolerate routine washing with hand soap and water, allowing it to be cleaned conveniently alongside the rest of the hand.
d. Competition:
- The previous prosthetic finger design consists of multiple articulated segments corresponding to the proximal, middle, and distal phalanges, with hinge joints aligned to the anatomical proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints. Flexion at the PIP joint serves as the primary driver of motion, activating a cable-driven mechanism that increases tension as the joint bends and actively flexes the DIP joint. A torsion spring integrated at the DIP joint provides passive extension when cable tension is released, returning the finger to its resting position. This combination of cable-actuated flexion and spring-assisted extension enables controlled articulation without the need for motors, while closely mimicking natural coordination between the PIP and DIP joints. The design improves realism during grasping tasks and reduces user effort through mechanical assistance. Additionally, the concept highlights the importance of anatomically aligned hinge joints and demonstrates the effectiveness of passive spring mechanisms in lowering operational effort. The internal components can be concealed beneath a cosmetic silicone covering, supporting both functional performance and a natural appearance, and providing relevant precedent for adjacent-finger-driven prosthetic concepts [17 ].
- This project describes a body-powered prosthetic finger that flexes in coordination with an adjacent intact finger using a tendon-like string mechanism instead of motors or electronics. The prosthetic features a segmented structure that approximates natural PIP and DIP joint motion, with rigid internal components providing structural support and flexible TPU elements enabling smooth, compliant When the neighboring finger flexes, tension in the internal string causes the prosthetic finger to move simultaneously, creating a passive, intuitive control system with low activation force. Designed for
low-cost 3D printing and rapid prototyping, the system demonstrates that
adjacent-finger-driven actuation is a feasible and effective strategy. It highlights the advantages of simple mechanical coupling, a minimal-part design, and the integration of rigid and compliant materials to achieve natural motion, providing a practical baseline for further design refinement [18 ].
- This prototype utilized a gear-based mechanism consisting of two partial gears and two full gears connected by pins to produce articulated finger Testing showed that the
design exceeded compressive strength requirements, experienced minimal degradation during cycle testing, and achieved an anatomically accurate range of motion at the PIP joint. However, the mechanism was relatively bulky, with gear diameters limiting opportunities for compact redesign. The DIP joint motion differed noticeably from that of a natural finger, and the design was difficult to scale for different finger sizes. Despite these limitations, the prototype provides a strong foundation for further development.
Future work could focus on refining the geometry to improve anatomical accuracy and developing parametric design software that allows finger dimensions to be input and automatically scaled, increasing adaptability and usability across a wider range of users [19 ].
References
- -O. Sandu and I. Doroftei, “Biomechanics-Driven Development of Prosthetic Fingers: A Two-Phalanx Approach,” BIPMF, vol. 71, no. 1–2, pp. 15–26, Oct. 2025, doi: 10.2478/bipmf-2025-0002.
- Liu, M. Van, Z. Chen, J. Angeles, and C. Chen, “A novel prosthetic finger design with high load-carrying capacity,” Mechanism and Machine Theory, vol. 156, p. 104121, Feb. 2021, doi: 10.1016/j.mechmachtheory.2020.104121.
- Bovenzi, A. J. L. Welsh, A. D. Vedova, and M. J. Griffin, “Acute effects of force and vibration on finger blood flow,” Occup Environ Med, vol. 63, no. 2, pp. 84–91, Feb. 2006, doi: 10.1136/oem.2004.019703.
- ISO 10993-10: Biological evaluation of medical devices — Part 10: Tests for irritation and skin sensitization, ISO, 2021.
- “Design of novel test rig for prosthetic finger distal interphalangeal and phalanx ” Accessed: Jan. 29, 2026. [Online]. Available:https://oce-ovid-com.ezproxy.library.wisc.edu/article/00006479-202504000-00010/PDF
- “Custom Fingers Prosthetic for Natural Appearance.” Accessed: Feb. 05, 2026. [Online].
- “3D Printing in Prosthetics: History, Benefits, and ” Accessed: Feb. 05, 2026. [Online]. Available: https://www.xometry.com/resources/3d-printing/3d-printing-in-prosthetics/
- “Skin Temperature – an overview | ScienceDirect Topics.” Accessed: Feb. 05, 2026. [Online]. Available: https://www-sciencedirect-com.ezproxy.library.wisc.edu/topics/immunology-and-microbiology/skin-temperature
- E. Bernard and M. F. Foley, “Upper acceptable surface temperature for prolonged hand contact,” International Journal of Industrial Ergonomics, vol. 11, no. 1, pp. 29–36, Jan. 1993, doi:
10.1016/0169-8141(93)90052-F.
- Ross, “3D Printed Prosthetics: Manufacturing Process, Materials, and Types,” Thomasnet.com, Oct. 23, 2023. https://www.thomasnet.com/insights/3d-printed-prosthetics/
- Yabuki et al., “Development of new cosmetic gloves for myoelectric prosthetic hand using superelastic rubber,” Robotics and Autonomous Systems, vol. 111, pp. 31–43, Jan. 2019, doi: https://doi.org/10.1016/j.robot.2018.09.004.
- “Artificial finger price & cost: Understanding index finger prosthetics,” finger prosthetic,
- “Silicone materials,” Products – Silicone Materials – Polytek Development , https://polytek.com/products/silicone/?page=1 (accessed Sep. 17, 2025).
- FDA, “List of Medical Devices by Product Code,”
- S. Food and Drug Administration, “Classify Your Medical Device,” FDA, Jan. 15, 2026.
- ISO 8549-1:2020, Prosthetics and orthotics — Vocabulary — Part 1: General terms for external limb prostheses and external orthoses, International Organization for Standardization, Geneva, Switzerland, 2020. [Online]. Available:https://standards.iteh.ai/catalog/standards/iso/dcd7023f-6561-47ec-937c-028d2b513315/iso-8549-1-2020. :content Reference[oaicite:0]{index=0}
- J. Hahne, “Finger prosthetic,” U.S. Patent Application US20210022888A1, Jan. 28, 2021.
- University of California, Berkeley, Engineering Design Group, “Body-powered finger prosthetic design,” student design report, Berkeley, CA, USA, 2023.
- Gkionoul Ntelı Chatzıoglou, Yelda Pınar, and Figen Govsa, “Biometric analysis hand parameters in young adults for prosthetic hand and ergonomic product applications,” Anatomy & Cell Biology, Feb. 2024, doi: https://doi.org/10.5115/acb.23.310.
Related News Articles

Magnet Retained Nasal Prosthesis Created in San Francisco
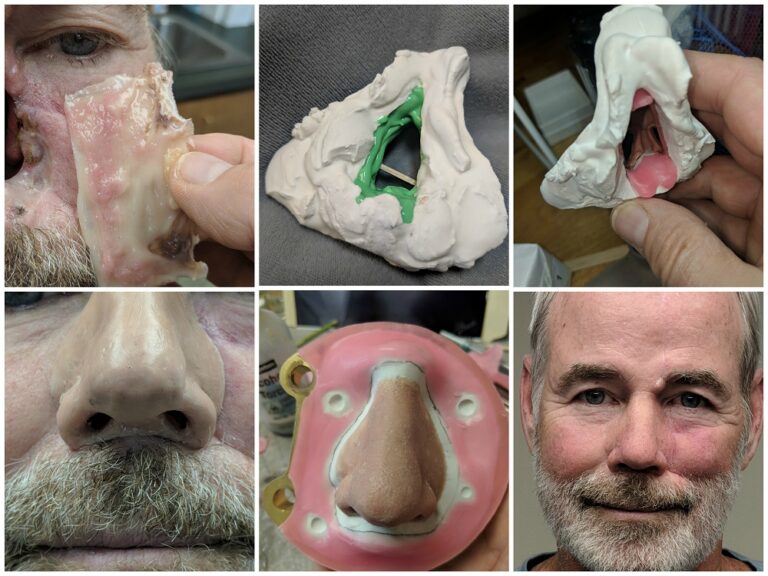
Easy-to-Wear Nasal Prosthesis for West Virginian
